

Health systems continue to face mounting profitability pressures. In response, system formation, growth and cost-cutting strategies have accelerated the need for strong physician alignment. Effective physician partnerships require solid, multifactor alignment in three areas:
- Clinical activity — Actively building systems of care needed to deliver the highest quality and lowest costs within the health system
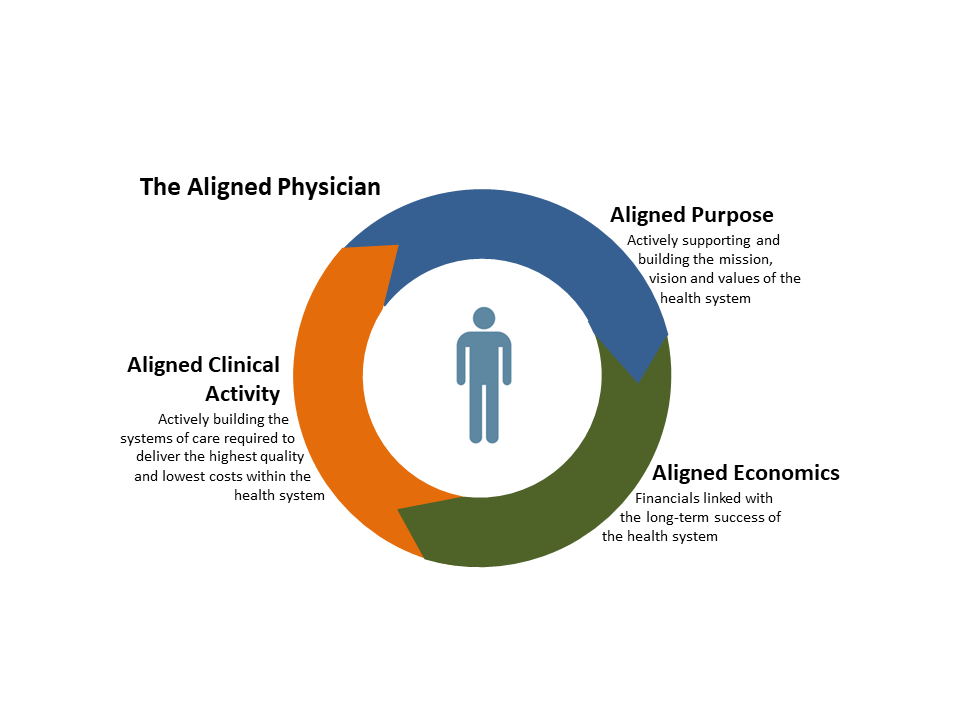
- Purpose — Actively supporting and building the mission, vision and values of the health system and expending energy to promote a common culture
- Economic — Financials linked to the long-term success of the health system
This content is sponsored by Health System Advisors.
The mix and extent of alignment needed will vary by situation. However, even with structural integration (e.g., employment), all three forms of alignment must exist to create a "unified whole" where:
- The providers' actions and activities are aligned with the health system's efforts (aligned clinical activity)1
- The providers' values and aspirations are consistent with the health system's mission, vision and values (aligned purpose)
- The providers finances are linked with the health system's long-term success (aligned economics)
How can the health system create physician interest in alignment and integration?
Health systems can create physician alignment with three types of actions:
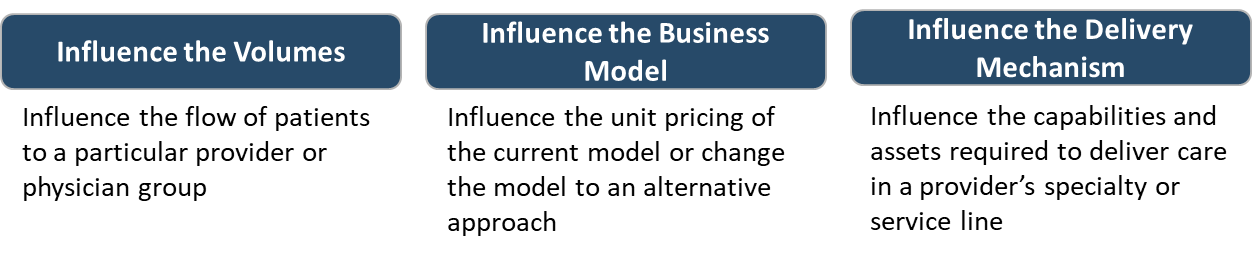
Influencing the Specialty Physician Group's Volumes
There are two major ways to influence a specialty physician or group's volume:
- Recapture the patient relationship
- Use payor relationships to channel patients with economic incentives
Recapture the Patient Relationship
Decades ago, the patient was as tied to the hospital as he was to the physician. Today there is often little patient connection to a specific hospital, especially within ambulatory services, which account for nearly 97% of all healthcare activity.
However, two trends can be used to the health system's advantage:
- Demand for and ability to coordinate care is increasing.
- The relationship between the physician and patient is declining.
Health systems are coordinating care better in part because of the proliferation of primary care employment. Coordination improves care and has the added benefit of channeling referrals to a set of physicians or group. To access these referrals, specialty providers must be in-network and can be partially influenced by the health system.
In the last five years, most health systems have focused on moving their employed primary care providers from aggregation to assimilation and integration.2 As a result, the average total in-network referral rates by employed primary care providers exceed 75% making it a reasonably effective tool for influencing specialists.
It is, however, an expensive approach to influencing volumes with subsidies of more than $100,000 per provider per year.
Additionally, the employment model's effectiveness is declining as the physician-patient relationship weakens. Easy access to basic clinical information, alternative channels of care and the increasing desire to have services delivered how, when and where the individual wants are reducing patients' dependence on a specific physician relationship.
A large (20%) and growing percentage of the population has traded the traditional physician-patient relationship for the convenience and access urgent care offers.3 Evidence of this trade-off is seen in the growth of urgent care centers compared to traditional primary care practices. Virtual, retail, concierge and other segmentation channels are attracting patients and serving as a substitute primary care channel.4,5
Health Systems that want to influence specialty physician volumes are using both primary care employment and alternative channel development to recapture the patient relationships.
Develop Payer Relationships
An alternative to capturing the patient relationship is to use economic incentives. This typically amounts to buying volume through narrowed insurance networks. By negotiating the hospital costs in exchange for payor-channeled volumes, the health system can exercise control over its specialty providers through the narrowed network referrals.
While in theory, the health system could develop the payor relationship through reducing total cost of care, this either directly or indirectly usually becomes an issue of unit pricing. As a result, the health system must balance the pricing leverage it has with the excess fixed capacity it could fill in the short-term.
Influence the Specialty Physician's Business Model
A second way to effect physician alignment change is to influence the specialty physician's business model. This could occur in at least three ways:
- Change the revenue per unit of work
- Monetize value already created but not yet monetized
- Shift the payment mechanism
Changing the Unit Price
By virtue of their size and large fixed-asset base, health systems can impact pricing for the physician and ambulatory platforms.
Historically, the health systems have worked with insurance negotiations to benefit the hospital and inpatient service pricing model. Given the ability for smaller firms to be more competitively nimble, there is logic to maintaining the strongest pricing where there are the largest barriers to entry.
Nevertheless, in an age where health systems are actively working to integrate the continuum, it is becoming less important where the profits are taken in the continuum. As such, insurer negotiations could be structured to better benefit specific parts of the continuum, thereby creating incentives for private practice physicians who operate in that area to integrate and capture better pricing.
More traditionally, the health system's clinically integrated network can create better pricing considering the scale and scope of services it offers the market.
In either case, the health system often has some indirect influence over the revenue per work unit created by the specialty physicians.
Monetize Value Already Created
Insurers have more recently been willing to pay for care management and other provider activities that reduce unnecessary care utilization. Often the services are already being provided by the group. However, these small physician groups are not capable of documenting the performance and negotiating the monetization scheme.
By banding small physician groups together to form a physician-hospital organization or clinically integrated network, the health system can negotiate and implement the processes needed to monetize the value already being created in some groups.
Alternatively, joint ventures with proceduralists allow physicians to monetize the technical fee profits from the work they are already doing. However, this is generally at the expense of the hospital. Facilitating this process can differentiate business models, thereby adding value to the physician-hospital alignment equation.
Shift the Payment Mechanism
To shift the payment mechanism, the health system must have some control over the market and participation from the insurers by virtue of size or value. For instance, to control the value equation when shifting from activity-based services to value-based services, the business model must change to include a whole range of continuum activities.
Influence the Care Delivery Mechanism
The third way, and perhaps most pervasive way, that health systems have attempted to effect physician alignment is through influencing the care delivery mechanism. This strategy is particularly effective when most of the care is delivered through major hospital infrastructure and in a community with only one or few health system options.
Today, however, more care is provided outside the hospital's influence and through easily replicable infrastructure. This loss of monopoly over care delivery infrastructure is making it more difficult for any one organization to fully control the care delivery mechanism. Nevertheless, several actions can be effective:
- Corner the complex specialty or infrastructure
- Build a reputation linked to the facility rather than provider
- Lobby for regulation that limits competition
Corner the Complex Specialty or Infrastructure
To effectively corner the market in a specialty and any downstream, an organization must employ a large subset of the specialists in a specific program. This is especially true for specialties that cannot stand on their own and are used often by related specialties (e.g., colorectal surgery, oncology, neurosurgery).
Alternatively, the health system could capture a large subset of the specialty technical infrastructure required for a specific high acuity or complex program. For example, with the best ICU staff, infrastructure and supporting physicians, specialties that depend on a specialty ICU platform must work with the health system that owns the needed capability or infrastructure.
Build reputation for care linked to the facility
By bringing together multiple specialties, the health system can create a unified reputation across those multiple specialties. With this multispecialty reputation, the synergy between the specialties creates value for any one specialty. In turn, it also increases the health system's influence over those providers.
This synergy and its effects can be seen in the US New Specialty Honor Roll. In 2017, any given hospital had roughly a 2% likelihood of being ranked in one specialty. However, when ranked once, there was nearly a 60% chance another specialty would be ranked. When ranked twice, there was a 77% chance of being ranked in three specialties.
Lobby for Anti-Competitive Regulation
The third and perhaps most effective method of controlling the care delivery mechanism is to have regulators prohibit alternative care delivery options. For example, strong certificate of need regulation may make new investments in a particular care delivery platform more expensive or difficult. In effect, lobbying would support the existing health systems' control over access to infrastructure.
Summary
To more rapidly effect the needed physician alignment, health systems should consider all the tools they have available. Thinking about the tools in three categories--influence over volumes, influence of the business model and influence over the delivery mechanism--can provide useful insight into new ways to effect physician alignment. Moreover, when used appropriately, the health system can create the catalyst for stronger health system-physician alignment, thereby creating higher quality, less costly, and more coordinated care for communities.
Kate Lovrien and Luke C. Peterson are Principals at Health System Advisors. Health System Advisors advises health systems on their competitive market positioning. Our team of motivated, engaged, and inspired strategists brings analysis, insight, and expertise as we facilitate your teams to new ways of thinking and strategies that advance your organization.
References
1Difference between alignment and Integration described by the authors in a 2010 article "Physician Alignment or Physician Integration?" Kate Lovrien and Luke Peterson, Becker's Hospital Review, August 27, 2010
2Aggregate, Assimilate and Integrate — Successfully Building an Employed Physician Group" Kate Lovrien and Luke Peterson, Becker's Hospital Review, May 7 2013
3Health System Growth Using Urgent Care" BHR Staff, Becker's Hospital Review, December 11, 2017
4New Research Demonstrates Virtual Care's Impact on Patient Acquisition, Return on Investment" PR Newswire, April 18, 2018
5The Virtual Primary Healthcare Revolution: What Health Systems Need To Know" Jon Pearce and Luke Peterson, Becker's Hospital Review, February 3, 2014