

When my husband told me that 10 prominent health system CEO's committed to do 11 things about the healthcare crisis that is physician burnout, I was excited.
With health systems like Johns Hopkins Medicine, Vanderbilt University Hospitals and Clinics, Duke University in Durham, Partners HealthCare of Boston and even the hospital where both I and my eldest daughter were born, Sutter Health in Sacramento on the list, I expected to see evidence-based, experienced-informed solutions that would make real progress quickly.
If you're not aware of the physician burnout crisis, recent studies indicate that over half of all physicians are already experiencing at least one of three symptoms of burnout. Symptoms of burnout include emotional exhaustion, cynicism or detachment and a sense that they are not effective or their work is not meaningful. Physician burnout is a serious problem for a number of reasons including:
1. It is contributing to a growing shortage of physicians as they leave the practice of medicine because of burnout,
2. Physician suicides are occurring at the rate of about 400 physicians per year,
3. Enrollment in medical schools is down as the arduous and expensive road to becoming a physician becomes less attractive as incomes decline and respect and quality of life of physicians is viewed as less favorable than it was in the past,
4. Physicians experiencing burnout are more likely to make errors,
5. Physicians experiencing burnout are more likely to die prematurely from all causes,
6. Physicians experiencing burnout may adversely affect the teams that work with them as emotions can be contagious,
7. A study in 2012 indicated that 6 out of 10 physicians would leave the practice of medicine if they were financially able to do so,
8. Physician burnout adversely affects patient outcomes.1
Job burnout has specifically been associated with poor outcomes or increased risk in the following areas:
• Cardiovascular diseases2
• Type 2 diabetes3
• Sleep problems4,5
• Musculoskeletal pain
• Impaired fertility
• Mortality
• Alcoholism and drug abuse/addiction
• Higher rates of suicide
"In the Medscape Physician Lifestyle Report, 46% of all physicians responded that they had burnout, which is a substantial increase since the Medscape 2013 Lifestyle Report, in which burnout was reported in slightly under 40% of respondents."
The Becker's Hospital Review article about the CEOs commitments which pointed to three studies to support the impact of electronic health records (EHR), low autonomy (control over the work) and increased regulatory burdens as the cause of high physician burnout. All the studies focused on the environment physicians work in and not their psychological resources which is where a physician's ability to change the level of stress they experience is within their control. The following studies all treat physicians as if they are without the ability to apply effective coping tools to their situation to mitigate the stress they actually experience:
The RAND study only considered factors physicians cannot easily control or influence, "Broadly speaking, factors that influence physician satisfaction can be divided into three key categories: physician demographics, workplace factors and changes in the healthcare system."
A 2009 study published in the Annals of Internal Medicine reflects conditions before significant regulatory burdens were added to physician duties indicated, "More than one half of the physicians (53.1%) reported time pressure during office visits, 48.1% said their work pace was chaotic, 78.4% noted low control over their work and 26.5% reported burnout."
The third article was more recent and included a significantly larger sample size than the 2009 article, Relationship Between Clerical Burden and Characteristics of the Electronic Environment With Physician Burnout and Professional Satisfaction, published by Mayo Clinic Proceedings
Positing physician burnout as something someone else has control over reinforces the low sense of control over one's work (low autonomy) which is associated with increased burnout. This focus also reinforces an external locus of control, the sense that something outside oneself is in control. An internal locus of control, the belief that one's own actions affect the outcome is associated with good mental health, higher employee engagement, lower burnout, increased resilience and other pro-health outcomes. Approaching burnout as if physicians cannot do anything personally to change their situations could worsen their perception of the issues.
That is not to say that healthcare systems can't do things to change the situation. Healthcare systems can and should make changes, but those solutions are usually not quick to implement. On the other hand, increasing physician resilience and coping skills can be done fairly quickly.
To put it in healthcare terms, with 46% of physicians experiencing burnout (as well as many nurses) the healthcare system is hemorrhaging. It needs a tourniquet to keep it alive until surgery (changes to the system, regulatory burden and highly functioning team models of care) can be implemented. Teaching active coping skills and the new, evidence-based definition of the purpose and use of emotions is the perfect way to stop the hemorrhaging. It increases one's internal locus of control which lowers stress and increases proactive coping which has been shown to reduce burnout and increase engagement and resilience.
This is why I was disappointed as I read the list of action items. What was on it?
1. Consistently measure physician well-being.
Measuring burnout can be done with the Maslach Burnout Inventory that has been in use for decades. It is a simple tool that takes minutes to complete. They could also measure Quality of Life or Dr. Diener's Life Satisfaction measurement tool, all of which are well documented evidence-based tools, all of which take mere minutes to complete.
The problem with measurement is measurement doesn't change the outcome. If a physician is burned out, measuring it doesn't lessen the problem.
2. "Where possible" include physician well-being into organizational performance dashboards with financial and other performance metrics.
This seems to ignore the fact that physician burnout is already included in the measurements. Patient outcomes, patient satisfaction, physician errors, physician productivity and physician turnover all affect the financial viability of hospital systems. They have blinders on if they think there is a situation where physician well-being isn't already included in their performance and financial outcomes. This step would give them greater clarity but anyone who understands the impact of burnout on patient care and turnover would know the numbers already reflect the level of burnout within their organization. A system with low burnout levels will have better results in every category. This is well-documented in the research.
3. Measure and monitor the institutional costs of physician turnover, early retirement and reductions in clinical effort.
The problem is they should already know the institutional costs of physician turnover and measuring it does not decrease physician burnout. It redirects resources to measure things that could be spent easing administrative burdens on physicians.
4. Emphasize the value of leadership development for physicians and managers who lead physicians.
I have no problem with leadership development for anyone but leadership does not have a strong correlation with burnout. The following diagram illustrates the continuum between highly engaged and burnout. We can talk about burnout prevention by increasing engagement or via reducing burnout. They're two ends of the same continuum.
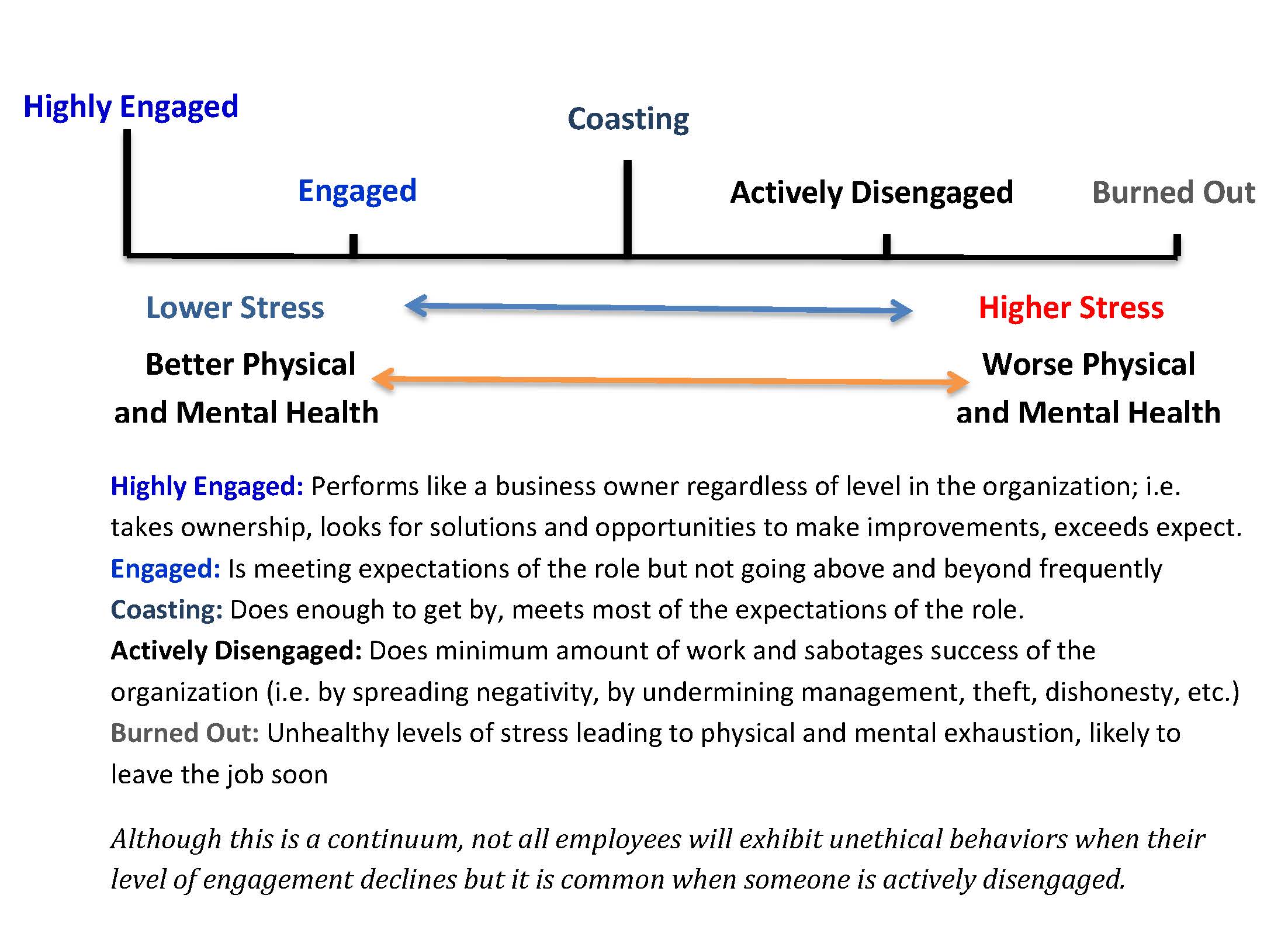
The research consistently shows a high correlation between employee engagement and an employee's core self-evaluations. An employee's core self-evaluations account for between 27 – 40% of engagement. On the other end of the continuum, high core self-evaluations have been reported as a factor that prevents against burnout in a number of studies. Core self-evaluations are a combination of the employee's self-esteem and evaluation of his or her own self-efficacy (competency).
The second largest factor that protects against burnout is active coping styles. Passive coping styles and low core self-evaluations are associated with increased burnout.
In Empowered Employees become Engaged Employees I explained why management can't get global engagement above 30% by giving positive, authentic feedback. It boils down to the fact that if an employee doesn't believe the compliment is deserved the mind makes up a back story that explains why the manager said what was said and the back story will probably portray the manager in a negative light, especially if the employee is negatively focused. Back stories are created by our minds to make sense of our experiences. They are created below our level of conscious awareness and are usually accepted as true by our conscious minds.
You have to look no further than social media to see how negatively focused our entire society has become. Or you can look at the published research and see that 10% of the population is depressed each year, 18% suffer from anxiety and a new Berkeley study indicates 20% have anger issues.
Leadership development won't solve the physician burnout crisis.
I'll discuss a solution that will work, shortly.
5. Understand and address the clerical burden and misallocation of work to physicians that contributes to the exhaustion component of burnout.
This will help. This should have been done before the government mandated Electronic Health Records (EHR) and tied payment reimbursements to them. Inputting data into a computer is not the practice of medicine. Whilst I see the benefit of a patient being able to present themselves anywhere and have the facility have access to the health records, when this is balanced against the massive increase in physician burnout and their exodus from the practice of medicine, I'm pretty sure it is better to have enough physicians than to have electronic health records.
Clerical assistance to input the records could ease the stress of spending time on the computer when physicians would be better utilized spending that time with patients and most would prefer to be with their patients.
6. Encourage collaborative, team-based care models to maximize physician expertise and delegate tasks to other team members.
This is great unless the team members they plan to delegate to will be nurses who are experiencing their own burnout issues and shortages of trained labor. There is also a need for training for teams so that there is less incivility on the teams, which is another problem reported frequently in the research, especially among nurses. Incivility is a symptom of low emotional state which could be an indicator of burnout.
7. Encourage policymakers to address the burdens imposed on healthcare by regulations that lead to redundancy, waste and inefficiency in healthcare environments.
I agree wholeheartedly with this one as a goal. It is not a quick fix and for the 46% of physicians who are currently burned out, help from this goal may come too late.
8. Support the AMA and other national organizations to work with regulators and tech companies to improve the circumstances and support healthcare solutions for everyone.
I agree with this but, again, it is not a quick fix and may be too late for many physicians who are already experiencing burnout. I would also have preferred that it mentioned evidence-based solutions. We have a tremendous amount of research that highlights solutions to this and many other problems our society isn't addressing using best practices.
9. Encourage and support the AMA and other organizations that are developing initiatives to make progress in this area by sharing best practices.
I agree but I would, again, mention looking to the research that already exists to identify potential avenues.
Research that talks about core self-evaluations often makes an erroneous assumption that core self-evaluations are fixed beliefs/conclusions about the self. This is not true. The Smart WayTM program we offer provides tools and knowledge that increases core self-evaluations. If they attempt to address the solution and rule out a viable one (improving core self-evaluations) simply because older methods failed to have an impact on core self-evaluations they miss a solution that would provide immediate benefits that would increase over time as physicians gained proficiency with the skills that lower stress and increase engagement.
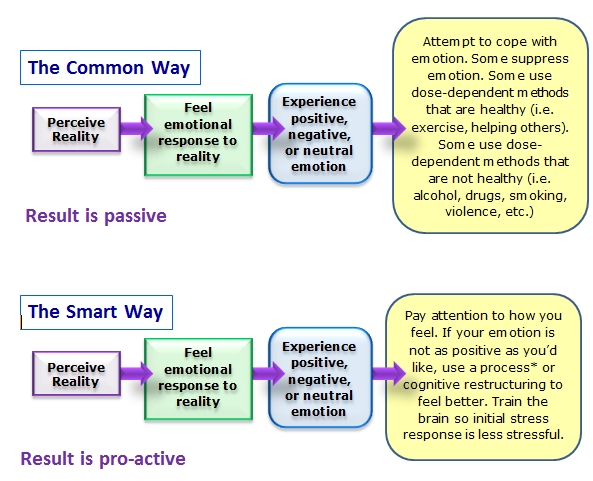
The Smart WayTM includes a variety of processes that can be used to change one's perception of reality. The best process depends on the emotion an individual is experiencing when the process is utilized. This is a positive approach model. It does not involve suppression. Rather, it empowers the individual with the ability to change perceptions until the emotional response improves.
Negative emotions are experienced and are viewed as a signal that some work is to be done relative to perception. There is no reason to steep in the negative emotion nor is there any benefit in doing so. The result is individual, in-the-moment control over emotion. The long-term result is increased optimism (positivity) that makes the first response to situations less stressful. Unlike most recommended ways to feel better, The Smart WayTM is not dose-dependent. Once perception changes, the next time the person thinks about the same subject their emotional response is better than it was before they took proactive steps to change their perception and sense of empowerment.
The Smart WayTM increases active coping and provides a framework that individuals can use to increase their core self-evaluations. It is more powerful and flexible than mindfulness alone.
Items #10 and #11 are good moves.
As I review this commitment to improve 11 areas in its entirety it has the same basic problem that is preventing us from implementing many good, evidence-based, experience-informed solutions. The entire list comes from a business perspective. There is no psychology mentioned at all despite the fact that burnout and stress are controlled by psychology. They were in their silo when they crafted this list.
Their intentions are good, I am sure. They don't know what they don't know. It's not as if the employee engagement industry is talking about core self-evaluations with employers despite the research demonstrating it is the single factor with the largest impact on employee engagement. They ignore it because they don't know the solution.
Who is the Henry Ford of our generation? When Henry Ford wanted an 8-cylinder engine his engineers repeatedly told him it was impossible. He told them not to come back until they had one. We all know how that story ended.
We can't turn the battleships (regulatory burdens) today but physicians can change their perspective and feel greater control over their work by learning tools that help them change their perspectives. Both should be done but let's use the low-hanging fruit first and get the people who take care of us, doctors and nurses, some relief now.
What action steps should be taken?
1. Teach every physician and nurse:
• Proactive coping skills
• To understand how their mind processes data and how to adjust the programming to improve their results (automates proactive coping)
• The new, evidence-based definition of the purpose and use of emotions
• The deep connection between emotions and behavior: This will help them improve their relationships at home and at work which provides further support that helps prevent burnout (This and proactive coping skills is the key to increasing core self-evaluations).
• Self-Compassion, which is proven to increase engagement and decrease burnout
• Techniques to overcome secondary trauma
• Strategies to live well when exposed to frequent death and dying
2. Develop the teams using the Positive Teams Coaching concept to further decrease workplace incivility
3. Items 1 – 11 from the list the CEOs developed and explore other cross-disciplinary solutions
In as little as one year we can turn the tide on both physician and nurse burnout. There would be a great side benefit in that the same skills they learn to prevent and recover from burnout would be of benefit to their patients whose lives are also stressful.
The following charts highlight many of the relationships between habits of thought and mindset and ultimate outcomes in important areas of physical and mental health.
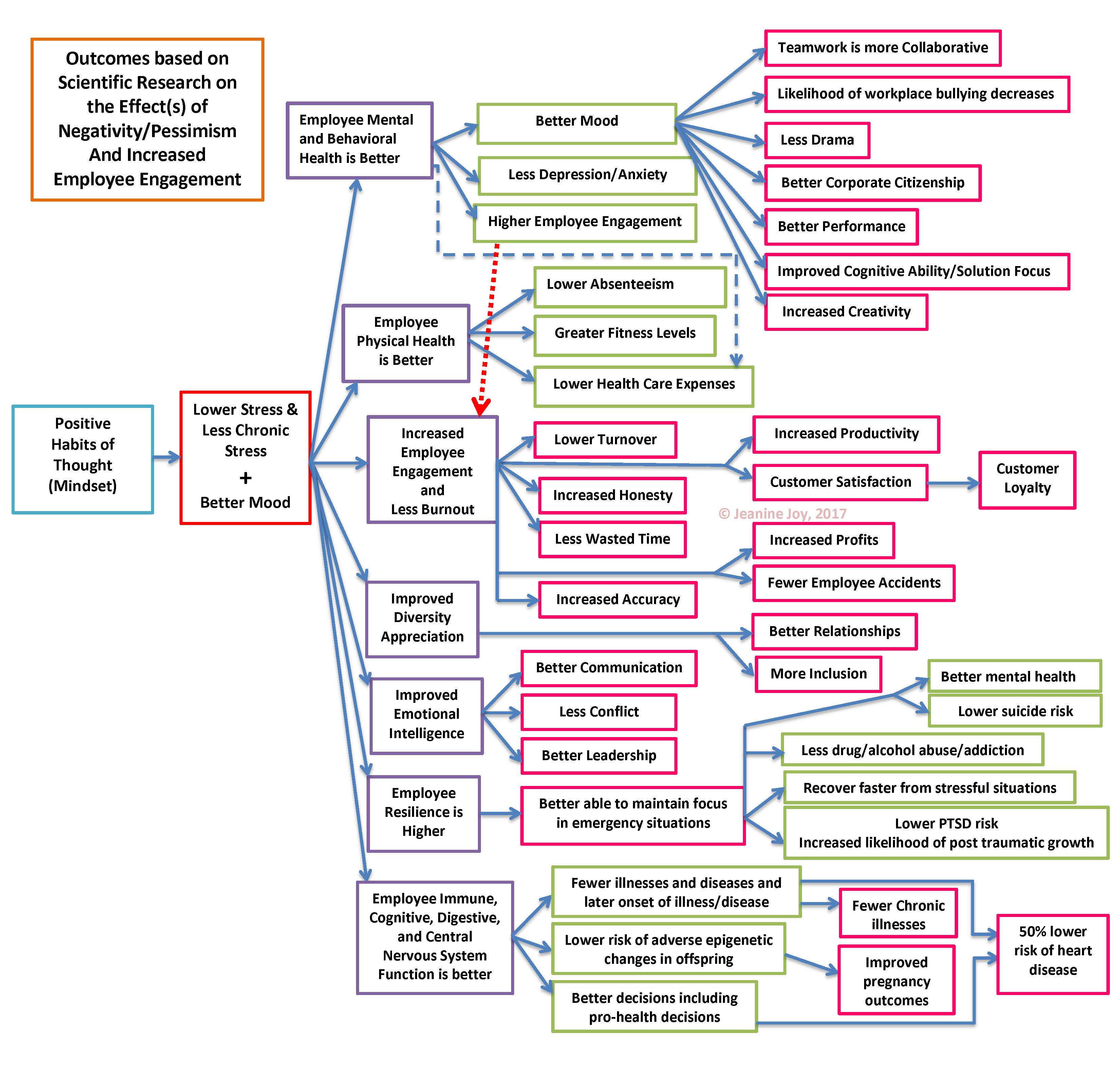
Citations supporting the above relationships are in one or more of my books and I will be happy to discuss them with any organization that wants to improve employee engagement and reduce burnout.
What are we waiting for?
If a doctor or nurse has ever helped you, please share this article.
[In compliance with the International Suicide Reporting Guidelines that save lives when they are followed, the following notice is provided: If you are considering harming yourself or someone else, there are people who want to help you. Call the National Suicide Prevention Hotline at 1-800-273-TALK (8255), call 911 (outside the United States call your local emergency number), or go to the nearest emergency room.]
BIO:
Dr. Joy wants people to know how easy it is for individuals and organizations to thrive more in every area. Every book and blog she writes, every training program she delivers and every speech she gives has the goal of helping people thrive more. Her solutions stem from the root cause of human thriving using solutions garnered from research that crosses silo's into every area that adds to the power of the solutions she shares. Thousands of people have learned to thrive more from her ideas and training programs. For more information contact her for a free consultation about how she can help you and your organization thrive more.
Bibliography
Armon, G., Shirom, A., Shapira, I., & Melamed, S. (2008). On the nature of burnout-insomnia relationships: a prospective study of employed adults. Journal of Psychosomatic Research, 65(1), 5-12.
Joy, Ph.D., J. (2016). Empowered Employees become Engaged Employees. Concord: Thrive More Now Publishing.
Melamed, S., Shirom, A., Toker, S., & Shapira, I. (2006). Burnout and risk of type 2 diabetes: a prospective study of apparently healthy employed persons. Psychosomatic Medicine, 68(6), 863-969.
Metlaine, A., Sauvet, F., Gomez-Merino, D., Elbaz, M., Delafosse, J. Y., Leger, D., et al. (2017). Association between insomnia symptoms, job strain and burnout syndrome: a cross-sectional survey of 1300 financial workers. BMJ Open, 13(7).
Peckham, C. (2015, January 26). Physician Burnout: It Just Keeps Getting Worse. Retrieved 2017, from Medscape: http://www.medscape.com/viewarticle/838437
Seligman,, M. (2006). Learned Optimism (Originally published 1991 ed.). New York: Simon & Schuster.
Shanafelt, T., & Dyrbye, L. (2012). Oncologist burnout: causes, consequences, and responses. Clinical Oncology, 30(11), 1235-1241.
Toker, S., Melamed, S., Berliner, S., Zeltser, D., & Shapira, I. (2012, October). Burnout and risk of coronary heart disease: a prospective study of 8838 employees. Psychosomatic Medicine, 74(8), 840-847.
Note: The original article, 10 prominent health system CEOs: Physician burnout is a public health crisis—here are 11 things we commit to do about it, was published by Becker's Hospital Review. This article is published under fair use in the way a book review can quote from the book. I have paraphrased the numbered items below from their article in order to comment upon them. All other content is my own. For exact quotes of the numbered items, please see Becker's Hospital Review.
1 (Shanafelt & Dyrbye, 2012)
2 (Toker, Melamed, Berliner, Zeltser, & Shapira, 2012)
3 (Melamed, Shirom, Toker, & Shapira, 2006)
4 (Armon, Shirom, Shapira, & Melamed, 2008)
5 (Metlaine, et al., 2017)
6 (Peckham, 2015)
7 (Seligman,, 2006)
The views, opinions and positions expressed within these guest posts are those of the author alone and do not represent those of Becker's Hospital Review/Becker's Healthcare. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them.