

Provider organizations completed reporting for the 2014 Medicare Physician Quality Reporting System (PQRS) in the first quarter of 2015, where many scrambled in the final weeks and days to gather, organize and submit their data to CMS. And yet, with those vivid memories still fresh in mind, activities for the current 2015 PQRS performance year have already begun.
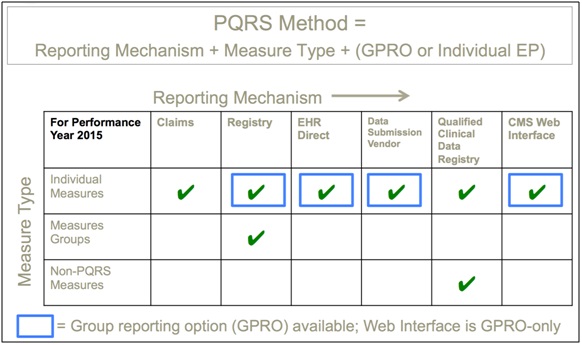
Organizations have now moved onto meeting the next PQRS deadline by June 30th, declaring to CMS what Group Practice Reporting Option (GPRO) reporting method, if any, to use for 2015. GPRO methods enable a group of providers, as identified by a common tax ID or "TIN", to aggregate their PQRS measure data into a single set of group-level measures to submit to CMS, rather than reporting providers individually. The declaration to CMS of which, if any, GPRO method to use is irreversible after June 30th. Furthermore, there are 11 different options across GPRO and individual-provider reporting methods to choose from (see the graphic below). Selecting the optimal reporting method with confidence and transparency to the pros and cons of different methods can be complex and daunting. For instance, it is time-consuming to read and apply the annually-updated PQRS and associated Value-Based Payment Modifier (VBM) programs to make the best GPRO decision tailored to your organization's situation.
The stakes are high. Combined incentives and penalties for the 2015 PQRS and VBM programs can swing from +4% down to -6% of Medicare Part B payments to providers. In particular, PQRS measure values largely determine whether an organization falls within the high (+2% incentive), medium (neutral impact), or low (-2% penalty) VBM quality tiers.
However, it has been demonstrated in the field that PQRS measure performance can vary greatly depending upon which reporting method you choose. For example, forgoing a GPRO method and opting for individual-provider reporting may cause an organization to fall into a lower VBM quality tier, thereby costing thousands, if not millions, in Part B reimbursement dollars. Even worse, selecting a reporting method that turns out to be unsupportable by your EHR vendor, infrastructure or staffing can result in the -6% maximum penalty for non-reporting.
5 Tips to optimize your June 30th GPRO decision. Even with limited time from now until the June 30th CMS deadline, there are some things you can do to make a better-informed decision about what GPRO method, if any, to declare to CMS:
1. Document the pros and cons of different GPRO and individual-provider methods to socialize with the decision-making team at your organization. Providing transparency to the decision process can align stakeholder support behind a decision that is rarely without risk or uncertainty. Ensure that your understanding of the relevant PQRS methods is accurate by consulting the authoritative CMS guides (good starting points are the 2015 GPRO criteria and the 2015 PQRS implementation guide or experts familiar with the 2015 rules who also have PQRS field experience). Explore and outline the tradeoffs among different reporting methods. For example, choosing GPRO for a large provider group may be administratively simpler than reporting providers individually. However, choosing GPRO for groups each with more than 100 providers requires that the Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) for PQRS patient satisfaction survey be conducted at an additional cost to the organization (as CMS is no longer subsidizing surveys). Documenting these tradeoffs and the logic behind your GPRO decision not only aligns the organization, but also makes it progressively easier to predict and make your GPRO decision in subsequent years. Many organizations will be best served re-visiting their GPRO decision each year as the rules and the organization's profile and infrastructure change.
2. Check to what extent your Electronic Health Record (EHR) or other necessary health IT systems will support your chosen GPRO reporting method. Last year, some provider organizations chose a reporting method their EHR vendor did not support. For those choosing the GPRO EHR Direct or Data Submission Vendor (DSV) methods, check with your EHR vendor(s) to determine when they expect their clinical quality measures (CQMs) calculations to be upgraded to the July 2014 version of the CQMs required for the 2015 PQRS (2014 PQRS used the older June 2013 version). In addition, check whether your EHR vendor(s) has tested its standard CQMs export file known as Quality Reporting Document Architecture Category III (QRDA III), using the PQRS file submission testing tool known as the Submission Engine Validation Tool, and not simply against the file standard used for EHR certification.
3. Beware of hidden administrative burdens and drawbacks of PQRS reporting methods. For example, the GPRO web interface method may seem very attractive due to only having to report on 248 patient beneficiaries. However, some organizations have found that the internal cost to extract and input the required data has eroded much, if not all of the financial upside of PQRS reporting. For the PQRS registry method, be sure to plan for staffing and time to perform the data extraction required by registry vendors, most of whom charge extra to take on that work. Factor these hidden costs into how you evaluate the return-on-investment of each possible reporting method.
4. Consider how to monitor performance of PQRS measures for your chosen GPRO or individual-provider reporting method. There can be drastic impacts to your organization's VBM quality score and, thereby, its Medicare reimbursement, based upon how your PQRS measures compare to CMS national benchmarks (e.g., the 2014 PQRS benchmarks for VBM). Each reporting method may involve calculating PQRS measure values in different ways, which impacts your options for monitoring measure performance throughout the year leading up to the submission season. For example, the EHR Direct and DSV methods utilize the CQMs, which may be monitored using EHR or 3rd-party dashboards and reporting tools. On the other hand, the web interface or registry PQRS measures may be more difficult to monitor in terms of how patient data needs to be extracted and handled under these methods.
5. In advance of June 30, 2015, review and prepare the information required by CMS to declare your GPRO reporting method. Don't wait until the last minute to acquire the login credentials and information needed to submit your GPRO decision to CMS. There may be items requiring lead time, which you may not have the luxury of completing if the deadline is too near. Consult and understand what's required by CMS, then log in to the Physician Value-PQRS (PV-PQRS) Registration System to directly confirm that you have the information you need to make a complete and valid declaration. For example, you must specify which size tier (2 - 24, 25 – 99, or 100+ PQRS-eligible providers) each provider group (as identified by Taxpayer Identification Number or TIN) falls into. This requires applying the 2015 PQRS eligibility rules to your provider roster to ensure you are making a truthful declaration.
Most important is to immediately start the decision process if you haven't already. Do not leave to "what seems right" in choosing your GPRO method or in forgoing GPRO in favor of reporting providers individually. It's too easy to mistakenly choose a sub-optimal or even infeasible reporting method that could result in large penalties. However, with some deliberate planning and research, you can make the June 30, 2015 decision with confidence and transparency for your organization.
Tom S. Lee, Ph.D., is the Founder and CEO of SA Ignite. You can send him comments and/or questions by email: tom@saignite.com.
The views, opinions and positions expressed within these guest posts are those of the author alone and do not represent those of Becker's Hospital Review/Becker's Healthcare. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them.