
In an effort to hold hospitals and providers more accountable for the quality and cost of care, CMS announced in early July 2015 the rollout of a bundled payment model for hip and knee replacement patients.
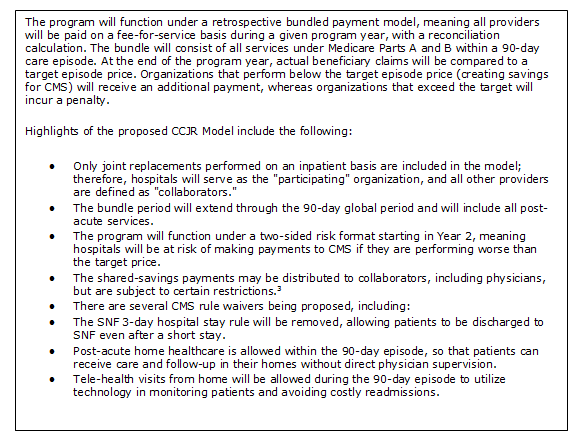
The Comprehensive Care for Joint Replacement Model, which specifically targets MS-DRG 469 and MS-DRG 470 patients, goes into effect in 75 selected markets beginning in January 2016 and will be effective for 5 years.1 In its proposal, CMS will make participation in the CCJR Model mandatory for hospitals in the respective MSAs.2
Many organizations may be unfamiliar with bundles and therefore unprepared to optimize care and reimbursement under the CCJR Model. For organizations developing a joint replacement bundle for the first time, here are four key factors that must be in place to ensure a successful program.
Appropriate physician alignment
Crucial to the success of a joint replacement bundled payment program is ensuring buy-in and participation from local orthopedic surgeons. Coordination with physicians who perform a significant volume of the procedures at the hospital seems self-evident but is often overlooked. A bundled program will be most successful when the physicians are fully aligned, because they can directly impact care management and drive cost savings in several areas:
- Minimize variation in surgical and follow-up protocols to reduce acute-care costs.
- Standardize supplies to keep costs low and maintain margins.
- Follow post-acute care treatment protocols to reduce readmission rates and unnecessary utilization, reducing the total cost of care for a joint replacement episode.
Traditionally, provider alignment through professional service, gain-sharing and comanagement agreements is codified in contracts that are governed by several regulatory requirements. The CCJR Model is proposing a slightly less stringent set of rules for collaborator agreements. The funds flow for these agreements is capped in terms of the value of payments, but the underlying metrics and earning mechanisms have more flexibility. Under the CCJR Model, it is imperative that agreements be reached with preferred collaborators in order to effectively manage care across the entire 90-day episode
Clear patient care plan
Managing patient care and monitoring overall program performance requires a clear understanding of the patient care plan. The plan guides all care team members across the entire episode of care, and deviation should only occur when there is agreement by the providers. The most successful hospitals maintain strong case management expertise specific to joint replacements. There are several care transitions during a joint replacement episode that, if not managed well, can result in additional utilization that may be costly, including emergency department visits, readmissions, unwarranted use of a higher-acuity care site and duplicative services. Several keys to the patient care plan include:
- A consistent surgical plan, including anesthesia, and postsurgical rehabilitation prior to discharge (e.g., surgical team, care plan, recovery, therapy plan).
- A post-acute rehabilitation plan and thresholds for discharge to various post-acute providers (e.g., home health, skilled nursing, outpatient therapy).
- Monitoring of patient recovery (e.g., pain, range of motion, strength and ADLs) through formal visits and other innovative methods such as tele-health visits and wearable devices.
Managing the care plan requires diligence, coordination and accountability among the providers and the patient.
Robust patient engagement
Patient engagement for joint replacements procedures has historically been limited to attendance at pre-surgical classes, compliance with medications and attendance at post-acute physical therapy. Programs that engage patients have shown greater success over programs without patient engagement mechanisms and the CCJR encourages providers to create new methods of patient engagement. The CCJR Model introduces several rule waivers—noted in the sidebar—that will allow greater flexibility for engaging patients. In addition, providers are allowed to offer patients direct incentives to become partners in their own care management (e.g., small financial incentives, use of technology such as tablet computers).
The intent of increased patient engagement is to improve quality and reduce any unnecessary utilization that may occur. Programs that use innovative approaches, including offering incentives for compliance and providing wearable or other monitoring devices, will maintain better control of the care process. Reducing variation such as readmissions, revisions and unnecessary emergency department visits will provide protection from the major cost drivers for joint replacement patients.
Bundle-specific operational skills
The last key to a successful program is to organize management and operations around the bundle. Executing a bundle requires an organization to approach patient care in a way that may not be consistent with historical practice. The most successful organizations evaluate their own ability to operationalize a bundle and conduct robust care management across the entire patient care process, beginning with the surgical plan, during the inpatient stay and throughout the recovery process. These skills are important in order to manage the financial risk associated with variation in care and avoid expensive negative outcomes. Organizations will likely need to cultivate relationships outside of their own four walls to successfully manage the 90 day episode. Key operating abilities will include:
- Tracking and monitoring patient performance consistently across the continuum (e.g., inpatient, post-acute facilities, physician activity).
- Sharing information consistently with providers, allowing for processes to be tracked and ensuring that patients are being cared for in a consistent fashion according to best practices.
- Implementing appropriate changes to the EHR and financial accounting systems in the form of new financial codes and proprietary procedure codes for care management, as necessary.
- Managing the supply chain to lower costs and optimize internal savings opportunities for the hospital.
These adjustments will allow for the accurate reporting of metrics to physicians, administrators and health plan partners. Regular monitoring of processes and utilization provides opportunities to change behavior and make cost-saving adjustments.
Use these four key factors as the basis for your organization's preparation for the CCJR Model. Without any one of these factors, your hospital will likely fall short of its goals of serving as a high-quality provider to patients in your service area and earning shared savings from the CCJR Model. For more information on how your organization can prepare for this model, please contact Jason Lee.
References
1 - The public comment period regarding this announcement is scheduled to end on September 8, 2015, and the final model will be published shortly thereafter. Note that all information regarding the model structure contained in this post is based on the proposed model, which is subject to change based on the input received during the public comment period.
2 - Exceptions include hospitals with low volume for MS-DRGs 469 and 470, critical access hospitals and hospitals already in the Bundled Payments for Care Improvement initiative Model 1 or the risk-bearing phase of Models 2 or 4 for joint replacement.
3 - The restrictions are similar to those in place for gain-sharing arrangements.
Jason Lee is a senior manager with ECG. In more than a decade as a healthcare industry consultant, Jason has worked with health systems nationwide to create hospital/physician alignment structures and optimize innovative reimbursement mechanisms. He is a nationally recognized speaker on managed care and health exchange issues.
The views, opinions and positions expressed within these guest posts are those of the author alone and do not represent those of Becker's Hospital Review/Becker's Healthcare. The accuracy, completeness and validity of any statements made within this article are not guaranteed. We accept no liability for any errors, omissions or representations. The copyright of this content belongs to the author and any liability with regards to infringement of intellectual property rights remains with them.