
Physician Relations programs developed out of need. In 1986 I was working with a healthcare organization that had developed and was managing a free-standing, specialized treatment center. After operating eight months and exhausting all traditional methods of marketing to both the public and referring physicians, the center still suffered lagging admissions. The corporate executive vice president of marketing — previously a marketing vice president for Johnson & Johnson with experience guiding the company's pharmaceutical and other product growth plans — suggested a plan of direct sales. The newly formed physician liaison team was able to implement the plan with overwhelming success!
Today, healthcare has become, of course, infinitely more complicated. Applying a basic referral-building mechanism across an entire health system is no longer enough to produce the anticipated results. It can, however, be extremely productive to apply the three winning principles cited above within the new strategies and structures described in the next section.
In the present healthcare environment, physician relations departments can be developed to fulfill the following objectives:
One can see that the full scope of responsibilities and activities required to reach these objectives would not be accomplished by one role or one position description. Some of these objectives require very different sets and levels of skills, knowledge, expertise, understanding and experience. Therefore, different, multiple roles are needed within the physician relations field team. We can no longer envision a one-size-fits-all physician liaison who performs all duties of physician interaction.
Some of these objectives may be more complex than ones your physician liaison staff has been charged with in the past. As you advance physician strategies to meet changing health system priorities, you will want to consider additional positions to assure a well-designed and appropriately managed and staffed physician relations team.
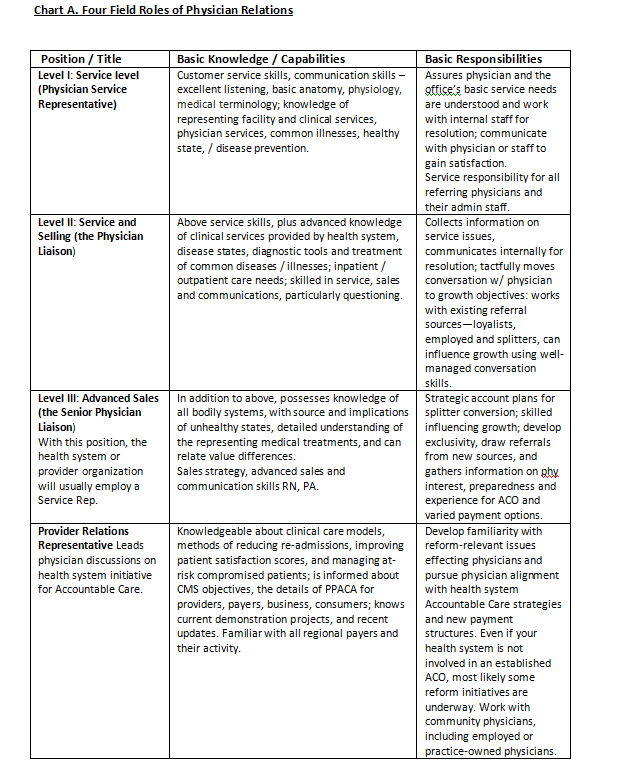
Physician relations managers can determine their staffing needs based on physician objectives to be met and the skills and expertise required to meet the objectives. Rather than thinking of one position description for all field representatives, consider the four positions (see Chart A) in the context of your department objectives, the health system's reform initiatives and current relationships with physicians.
Indeed, the prediction of many inpatient providers that reform efforts will lead to lower daily census could, inevitably, come true. There is, however, an advantage here: knowing about this inevitable decline gives the health system a chance to prepare for it through further physician relations.
Kathleen Harkins is principal of Harkins Associates, a healthcare business development and sales consulting/training firm. As a career-long healthcare strategist, seller, sales trainer, manager and company executive, Ms. Harkins has experience in several healthcare sectors — health insurance/managed care, capital equipment, professional services, information technology, hospitals and pharmaceutical. Prior to establishing the consulting and training firm 12 years ago, Ms. Harkins was employed as chief marketing officer for Progressions Health System, a managed inpatient and outpatient provider system; she also served as vice president of sales and marketing for Westmeade HealthCare, Inc.
The impact of healthcare reform on physician relations
Though in the last 26 years the healthcare industry has changed dramatically and has developed and implemented new physician-relations strategies, some of the principles that made our program in the 1980s a rousing success still apply today:- Everyone on the team — organization CEO, medical director, CFO, as well as the treatment center's physicians, clinicians and administrative staff — agreed to support the program utilizing sales-trained field staff to engage face-to-face with existing and potential referring physicians.
- Everyone — all member of the team cited above — was willing to learn and adapt as new information and experiences suggested a change in what had been planned.
- All team members were willing to fulfill any role or complete any tasks that needed doing.
Today, healthcare has become, of course, infinitely more complicated. Applying a basic referral-building mechanism across an entire health system is no longer enough to produce the anticipated results. It can, however, be extremely productive to apply the three winning principles cited above within the new strategies and structures described in the next section.
In the present healthcare environment, physician relations departments can be developed to fulfill the following objectives:
- Avoid losing exclusivity. Retain those physicians (and their exclusive referring patterns) who have been loyal to your hospital or health system.
- Provide "customer" service and issue resolution. Work with the physicians and practice staffs who have complaints or suggestions about common hospital services, such as delayed discharge notes, difficulty getting patients needed appointments, long waits on hold, specialists who do not return calls and a variety of other grievances.
- Understand community physicians, share information and influence. Understand community physicians and, where appropriate, share information on the health system services, diagnostic and surgical advances, new technology and outcomes; influence utilization of your services and facilities by current physicians, splitters and new physicians.
- Re-educate targeted, well-vetted physicians. Let them know about new care models, care management initiatives, payment systems and new procedures throughout the hospital, from admissions through discharge.
- Investigate interest and preparedness of community providers for accountable care. The physician relations department can take on at least partial responsibility for provider network development and work in cooperation with the medical staff office/credentialing office to share with community providers your system's accountable care organization expectations and identify other ACO activity within the community. Stay abreast of CMS policies and updates on ACOs.
One can see that the full scope of responsibilities and activities required to reach these objectives would not be accomplished by one role or one position description. Some of these objectives require very different sets and levels of skills, knowledge, expertise, understanding and experience. Therefore, different, multiple roles are needed within the physician relations field team. We can no longer envision a one-size-fits-all physician liaison who performs all duties of physician interaction.
Some of these objectives may be more complex than ones your physician liaison staff has been charged with in the past. As you advance physician strategies to meet changing health system priorities, you will want to consider additional positions to assure a well-designed and appropriately managed and staffed physician relations team.
Physician relations managers can determine their staffing needs based on physician objectives to be met and the skills and expertise required to meet the objectives. Rather than thinking of one position description for all field representatives, consider the four positions (see Chart A) in the context of your department objectives, the health system's reform initiatives and current relationships with physicians.
Physician conversation skills
In addition to re-thinking these roles and responsibilities, consider other important factors that have materialized since our early physician liaison experiences. We learned rather quickly that the often used pharmaceutical model of "contact and pitch" with physicians was not going to work for physician liaisons. Most traditional sales tactics can actually stifle good physician relationships. Newer more sophisticated models, such as Healthcare Consultative Selling™ for sales communication are far more effective.A reality for early adopters
Healthcare continues to be the battleground of change and challenge it's been for the past 30 years, but today the stakes are greater, technologies more complex, patients' conditions more complicated with more people requiring higher levels of care, and the costs infamously colossal. Even some of the forward-looking hospitals involved in shared savings programs via ACOs — those early adopters of Patient Protection and Affordable Care Act — are beginning to see inpatient days dwindle and a backlog of empty beds grow.Indeed, the prediction of many inpatient providers that reform efforts will lead to lower daily census could, inevitably, come true. There is, however, an advantage here: knowing about this inevitable decline gives the health system a chance to prepare for it through further physician relations.
Looking ahead
Some current realities are likely to remain into the immediate future:- Lack of trust between physician and hospitals. Competitive factors, service issues, CMS in-hospital and physician-office-based service reimbursement disparities, differences in daily business operations and other issues have impacted relationships between the two groups for years.
- Electronic health records are creating problems for physicians. A recent report shows that physicians who have implemented EHR solutions have found not a gain in profits but a loss.
- The long-term impact of healthcare reform on our country's economic condition is unknown and minimally beneficial in the foreseeable future.
- So far it seems hospital-led ACOs are focused on inpatient cost reductions, while those led by physicians are focused on ways of reducing outpatient costs, which is producing cost reductions in both areas. As ACOs evolve, and hospitals and community-based physicians work together, we'll likely see care coordination in the area of greatest risk to the patient — the transition from one level of care to the next.
- With the hope of individuals taking steps to improve our health, better coordination of improved quality, shorter inpatient stays and reduced clinical redundancies, it seems one likely potentiality is many more empty beds and, likely, fewer facilities. This scenario presents a case for continued, if not increased, competition among health systems. Therefore, the need for a strong physician relations function is likely to be with us for years to come.
Kathleen Harkins is principal of Harkins Associates, a healthcare business development and sales consulting/training firm. As a career-long healthcare strategist, seller, sales trainer, manager and company executive, Ms. Harkins has experience in several healthcare sectors — health insurance/managed care, capital equipment, professional services, information technology, hospitals and pharmaceutical. Prior to establishing the consulting and training firm 12 years ago, Ms. Harkins was employed as chief marketing officer for Progressions Health System, a managed inpatient and outpatient provider system; she also served as vice president of sales and marketing for Westmeade HealthCare, Inc.
More Articles on Physician Recruitment:
Improve Growth Outcomes by Aligning Marketing and Physician Relations Strategies
Is Your Organization's Physician Relations Team Centralized?
Increasing Hospital Referrals: Mastering the Sales Dialogue with Physicians